- ABSTRACT
A 28-year-old female patient with a brachyfacial biotype presents with a deep bite exacerbated by previous orthodontic treatment involving two upper extractions, which negatively impacted her lower facial vertical dimension. Cephalometric analysis confirmed a vertical skeletal discrepancy consistent with a skeletal-based anterior deep bite. The treatment plan involved a possible combined orthodontic-surgical approach, including bimaxillary surgery, that after weeks of thinking about it on the part of the patient, this option would be the last one. As a health professional, she seeks retreatment focusing on functional improvement and long-term stability. The current approach prioritizes vertical control and neuromuscular balance to address the compromised facial proportions and occlusal function. We currently find composite restorations in some interproximal areas, which have developed discoloration, further worsening the intraoral aesthetic appearance.
Palabra Clave: Neuromuscular Class II orthognathic surgery Anterior guidance
- INTRODUCTION
Deep bite malocclusion presents a complex therapeutic challenge that requires individualized diagnosis and biomechanically sound planning. A critical component in the management of deep bite is the evaluation of the patient’s facial biotype, which directly influences vertical control strategies and overall treatment planning.
For example, brachyfacial patients with low mandibular plane angles and strong musculature often exhibit reduced lower facial height and limited vertical adaptability, whereas dolichofacial individuals present increased vertical dimensions and require careful management to avoid worsening skeletal disproportions.
In this context, cephalometric analysis provides essential quantitative data—such as facial axis, mandibular plane angle, anterior facial height, and occlusal plane orientation—that guide the selection and direction of force systems used throughout treatment.
Beyond skeletal and dental considerations, it is important to recognize the role of neuromuscular stability in long-term retention. In particular, the absence of proper interincisal contact (anterior guidance) may compromise functional occlusion. At this point, an altered neuromuscular response involving the mesencephalic nucleus of the trigeminal nerve may be considered, potentially leading to parafunctions and relapse. Establishing and maintaining functional anterior guidance is therefore a key objective in achieving long-term stability in deep bite correction.
- CLINICAL AND CEPHALOMETRIC ASSESSMENT

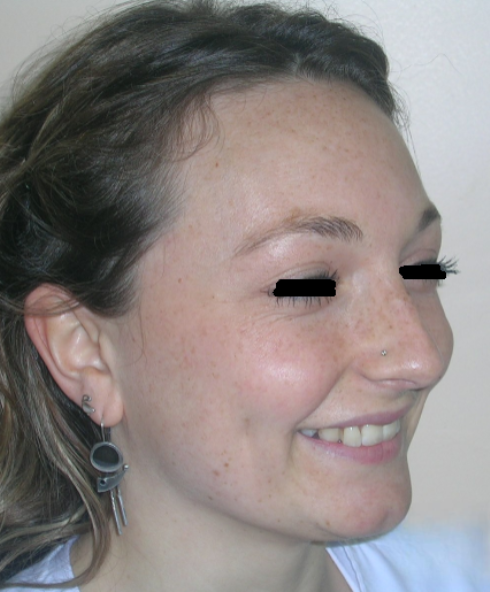

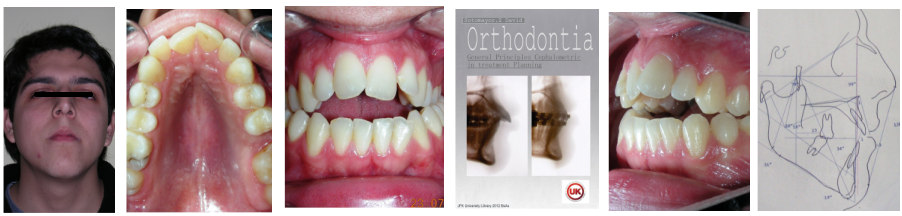
Clinical Findings:
Patient without asymmetries, relatively proportional face , only to mark the diminished lower facial third, slightly convex profile, marked masseteric muscles. At first intraoral sight vertical lack of coordination between the dental arches is observed. The maxillary incisors exhibit an exaggerated overbite, covering approximately 90% of the mandibular incisors.
Multiple diastemas are present across the entire maxillary arch, which aesthetically highlights the presence of a fixed lingual retention wire. Several interproximal composite ‘fillings’ are observed, all heavily pigmented , compromising both function and esthetics. There is coronal disto-inclination of the maxillary canines, along with altered root angulation (TIP), No coincidence dental midline deviated 2 mm. Relation Angle Class II molars and canine





Function: The patient exhibited significant functional deficiencies. Despite a skeletal pattern compatible with strong elevator musculature (brachyfacial), clinical examination revealed the absence of effective anterior guidance, with no incisal contact. Consequently, the patient lacked proper occlusal guidance pathways—a condition that may compromise both dynamic occlusal function and neuromuscular regulation.
This absence of anterior guidance and non-existent functional occlusal schemes (canine or group function) eliminated key proprioceptive stimuli necessary for physiologic muscle coordination and mandibular positioning. This is especially relevant in brachyfacial patients, who exhibit high resting and functional bite forces, and in whom the neuromuscular system relies heavily on occlusal input for calibration.
From a neurophysiological perspective, the mesencephalic nucleus of the trigeminal nerve plays a central role in proprioception and motor control of the masticatory system. This nucleus receives afferent signals from periodontal mechanoreceptors, muscle spindles (particularly in the masseter and temporalis), and temporomandibular joint receptors. The absence of consistent anterior contact likely reduced afferent input to this nucleus, leading to a disorganized neuromuscular pattern, excessive muscle tone, and possibly dysfunctional mandibular rest posture and parafunctional tendencies.
Facial biotype
Algebraic sum (+2 ) +( -1,6) + ( +1) + (+1,25 )+ (+1,5) = + 4,15 ÷ 5 = + 0,83 BRACHIFACIAL
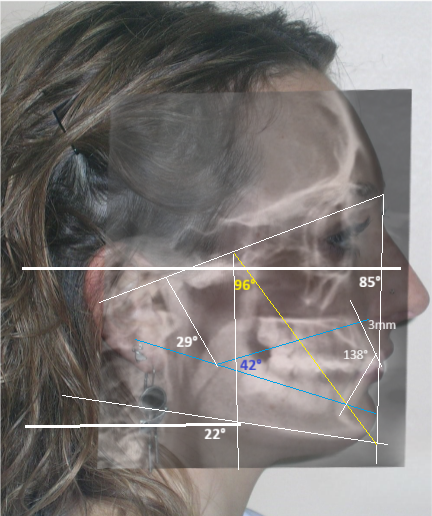
Cephalometric diagnosis
1,
| arameter | Patient (22yo) | Normal | Interpretation |
|---|---|---|---|
| Facial Axis | 96° | 90° ± 3° | increased , indicative of vertical growth pattern + Brachifacial |
| Facial Depth | 85° | 90°± 3° | reduced – dolichofacial tendency |
| Mandibular Plane Angle | 22° | 26° ± 4° | decreased +brachifacial tendency |
| Lower Facial Height | 42° | 47 ± 4° | decreased , short lower third+ Brachifacial |
| Convexity (A–N–Pog) | +3 mm | ±2 mm | Normal |
| Upper Incisor to A-Pog | 1 mm | 2–4 mm | Normal |
| Inclination lower Incisor | 20° | 22° | normal |
| Interincisal angle | 138° | 130° ± 6° | Increased – verical position of incisors |
| Maxillary–Mandibular plane angle (MM angle) | 26° ± 4° | ||
| Mandibular arc | 29° | 26 °± 2 | Increased +Brachifacial |
| Cranial deflection | 27° ± 4° |
Algebraic sum (+2 ) +( -1,6) + ( +1) + (+1,25 )+ (+1,5) = + 4,15 ÷ 5 = + 0,83 BRACHIFACIAL
Planning Considerations Following Facial Biotype Assessment
Once the brachyfacial skeletal pattern has been identified, an individualized treatment approach is developed, taking into account both skeletal and dental characteristics. This facial type is typically associated with a horizontal growth pattern, reduced lower facial height, aggravated by extractions of first premolars in previous treatment, and increased activity of the masticatory muscles, all of which must be carefully considered during biomechanical planning.
The most relevant cephalometric indicators in the evaluation of brachyfacial growth in this specific case include the Facial Axis and Lower Facial Height.
The treatment will aim to reduce the facial axis angle and increase the lower anterior facial height through controlled extrusion of the posterior segments. This vertical modification will help counteract the deep bite tendency typically observed in brachyfacial patterns. Once the vertical dimension is reestablished, space closure will be carried out using sectorized mechanics, allowing for precise control of tip and torque. Particular attention will be paid to the control of incisor position, as these patients often present with retroclined or overly upright incisors, which contribute to the deep bite and reduced incisal display. It is important to note that, in untreated patients distalization It would be our first option because it induces mandibular rotation in the counterclockwise direction. While this may be beneficial in brachyfacial or hypodivergent patterns, where increasing vertical dimension is necessary, it is generally contraindicated in dolichofacial patients due to the risk of worsening vertical excess and facial disproportions
Treatment plan
-
Removal of all interproximal restorations placed during previous treatment, in order to reestablish accurate proximal contacts and facilitate proper tooth movement.
-
Establishment of an anterior bite plane to achieve posterior disocclusion and allow for vertical development in the posterior segments.
-
Extrusion of posterior teeth to increase lower anterior facial height and reduce the facial axis angle, contributing to vertical correction of the deep bite. In accordance with one of the key principles of the bioprogressive philosophy—addressing malocclusion in a hierarchical sequence—this case prioritized correction of the vertical discrepancy (deep bite) before addressing the sagittal problem.
-
Control of tip and torque in the maxillary canines to ensure proper axial inclination and alignment within the arch.
-
Space closure with precise torque control, particularly in the anterior segments, to maintain ideal root positioning and achieve a stable occlusion.
- solved the sagittal and vertical problem, install sequence of continuous archwires
- Establish and maintain functional anterior guidance for proper disocclusion during excursive movements.
- Design a personalized retention strategy
Treatment phase
Following referral to the DMD the restorations were removed, the clinical scenario became significantly clearer after removal of the discolored interproximal fillings. With improved visibility and access, fixed orthodontic treatment was initiated by bonding metal brackets in the posterior segments using the Roth prescription. 022″ slot (Henry Schein®). Simultaneously, a removable anterior bite plate was delivered. The appliance was fabricated in acrylic and indicated for full-time wear, to be removed only for oral hygiene.




The purpose of the anterior bite plate is to disocclude the posterior segments and facilitate vertical dental development. With posterior disocclusion established, vertical elastics were prescribed in the posterior quadrants. The elastics selected were 3/16″ Heavy, delivering approximately 6.5 oz (≈185 g) of force, manufactured by the Brazilian company Morelli®. These auxiliaries aim to promote controlled extrusion of the posterior teeth as part of the vertical correction protocol in this brachyfacial case.
Sectional archwires were designed from tooth #16 to #13 and from #26 to #23 using . 017″ × .025″ Blue Elgiloy wires. This approach allowed for three-dimensional control of both maxillary canines in an early phase of treatment, as their roots were initially positioned against the buccal cortical plates.


This movement required the application of targeted buccal root torque to move the roots away from the cortical bone, which is characterized by low vascularity and high bone density. In addition, simultaneous distal root tip was applied to improve axial inclination and root positioning.
It is essential to consider the biological limitations of tooth movement when planning and executing such mechanics. Appropriate force systems must be selected to avoid iatrogenic effects and to respect the adaptive capacity of the periodontium under heavy anatomical constraints.

After achieving an increase in vertical dimension—specifically the lower anterior facial height—several key factors must be considered to prevent relapse, particularly the unintended intrusion of the posterior teeth.
One of the most critical elements is the reestablishment of proper interincisal contact through ideal incisor angulation. A target interincisal angle of approximately 130° is recommended, as this cephalometric parameter is crucial for achieving optimal anterior coupling and neuromuscular balance.


This angulation facilitates an appropriate functional response from the mesencephalic nucleus, which collect sensory information from receptors in the muscle spindles and the periodontal ligament, transmitting proprioceptive input to the motor nucleus of the trigeminal nerve, regulating muscle tone.
In this way, we aim to induce a neuromuscular ‘reset’ of muscle activity intensity, thereby reducing the need for non-permanent compensatory treatments such as botulinum toxin (Botox®) injections.
To achieve this biomechanical objective, a utility arch (Utility Retraction Arch with Maximum Torque) will be fabricated using Blue Elgiloy wire .017″ × .025″, previously dental aligned with Niti archwire 016″ x .016″ NiTi . This arch will deliver maximum lingual root torque , intrusion and retrusion with the ideal strength for the four maxillary incisors . The mechanics will be complemented with Class II elastics (3/16″, Medium force) to aid in anchorage control and directional force application. As the name implies, the utility arch offers precise three-dimensional control, particularly of incisor torque, effectively preparing the anterior segment for stable and functional contact. After addressing the vertical and sagittal discrepancies through the use of sectional and utility archwires, the case will proceed to the finishing and detailing phase using the full archwire sequence with pre-adjusted brackets. As previously mentioned, the system used follows the Roth prescription .022.
A progressive archwire sequence was used for finish with three-dimensional control.
-
.016″ NiTi round wire
-
.016″ × .016″ NiTi rectangular wire
- 019″ × .025″ Niti + Elastic chains to consolidate the closure of spaces, ensuring proper contact points and minimizing the risk of space reopening during the finishing phase
- 019″ × .025″ Braided + metal ligature to finalize and provide occlusal stability and optimizing tooth settling and intercuspation.






After 20 months of orthodontic treatment, the improvements are clearly evident. The anterior deep bite has been corrected, with proper incisal display and functional anterior guidance now established. Midlines have been aligned, spaces fully closed, and occlusal relationships significantly improved. The overall result reflects not only dental alignment but also enhanced vertical dimension and occlusal stability. The case is now ready for debonding
Finishing and Retention
The initially planned treatment duration was two years; however, full orthodontic objectives were achieved earlier than expected. In addition to meeting the primary goals outlined at the start of treatment, unexpected but favorable outcomes were observed and confirmed through cephalometric analysis.




Intraorally, beyond the successful correction of the deep overbite, one of the most remarkable results was the final positioning of the maxillary canines. Their angulation and inclination were fully restored to optimal values, contributing to both functional guidance and esthetic balance .The dental midlines were perfectly aligned, and a solid Class I relationship was established at the level of the premolars, ensuring proper occlusal interdigitation.






Upon completing the active treatment phase, a dual retention protocol was implemented. In the lower arch, a fixed retainer was placed from tooth #33 to #43 using twist-flex (supercable) wire , which had been heat-treated to eliminate its elasticity to ensure long-term stability.

In the upper arch, a combination of fixed and removable retention was used. The fixed retainer was extended from tooth #14 to #24—covering more than 60% of the dentition—deviating from the standard protocol. This approach was implemented following a shared decision-making process with the patient, she works in dentistry field and understood the implications of extended fixed retention. Additionally, a removable thermoformed Essix-type retainer was provided for nighttime wear.
From a cephalometric standpoint, an increase in facial depth was noted from 85° to 89° , indicating a forward repositioning of the mandible. This skeletal response occurred as a result of “unlocking” the anterior occlusion, which had previously been constrained by a deep bite.
The interincisal angle measured 131°, indicating optimal incisor angulation, which contributes to functional anterior guidance . The facial depth increased by mandibular repositioning and vertical changes Induced by posterior molar extrusion , resulting in minimal variation in the facial axis angle (from 96° to 95°) and lower anterior facial height (from 42° to 44°). This skeletal response not only preserved overall structural harmony, but also provided a notable esthetic benefit by enhancing lower facial projection and improving profile balance.
- CONCLUSION
Following comprehensive orthodontic treatment, the vertical discrepancy was corrected without the need for orthognathic surgery. The treatment approach focused on posterior extrusion rather than anterior intrusion,This strategy led to a clockwise movement. The success of these specific movements was achieved utilizing sectional archwires, which allowed for individualized control of torque and tip in each segment. This strategy allows problems to be sectored, maximizing treatment time. The cephalometric results show a slightly reduction in the facial axis angle and a increase in lower facial height. These skeletal and dental changes contributed to improved facial harmony, a more balanced lower facial third, and enhanced smile esthetics.
Functionally, the establishment of stable anterior incisal contacts played a critical role in promoting neuromuscular reprogramming of the mesencephalic nucleus of the trigeminal nerve, which is responsible for proprioceptive control of masticatory muscle tone. The newly established anterior guidance provided consistent, physiologic occlusal input, facilitating a reorganization of neuromuscular patterns and contributing to a more balanced and stable stomatognathic system.
REFERENCES:
1- Carpenter, R. H. S., & Reddi, B. Neurophysiology: A Conceptual Approach. 5th ed., Taylor & Francis / CRC Press, (2012).
2- Clinical investigation of botulinum toxin (prabotulinumtoxin A) for bruxism related to masseter muscle hypertrophy: A prospective study. Journal of Cranio-Maxillo-Facial Surgery. Kim, Y., et al. (2023).
3 – Gregoret, J., Tuber, E., Escobar, L. H., & Matos da Fonseca, A . Orthodontics and orthognathic surgery: Diagnosis and Planning. Amolca (2014).
4 – Contemporary Orthodontics — William R. Proffit, Henry W. Fields, Brent Larson & David M. Sarver. Elsevier. 6ª (2018)
5 – Systemized Orthodontic Treatment Mechanics —MBT- Richard P. McLaughlin, John C. Bennett, Hugo J. Trevisi. 1ª edición. Mosby, diciembre de (2001)
6 -Ricketts’ Bioprogressive: An Orthodontic Philosophy for Future Generations — Nekusuto Publishing, (2021)
7 – Orthodontic diagnosis and planning their roles in preventive and rehabilitative dentistry.Ricketts RM, Roth RH, Chaconas SJ, Schulhof RJ, Engel GA. 1 ed. Denver: Rocky Mountain; (1982).