

- RESUMEN
El objetivo de este caso clínico es demostrar la corrección de una mordida abierta anterior (MOA) con maxilar estrecho en un paciente adulto, considerando la respuesta de rotación anterior de la mandíbula.
Un paciente masculino de 22 años acudió a mi clínica de ortodoncia con el motivo de consulta: «No me gusta mi sonrisa y, al hablar, tiendo a expulsar saliva… ¡Ah! Y quiero poder morder una manzana», dijo con buen humor y actitud positiva.
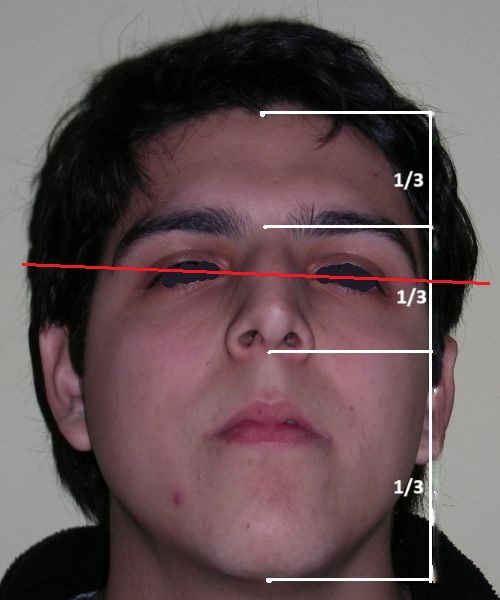
El examen clínico extraoral reveló una cara alargada verticalmente, con un tercio facial inferior aumentado. El perfil facial era ligeramente convexo, con una proyección deficiente del mentón. El examen intraoral mostró una mordida abierta anterior y una mordida cruzada posterior bilateral.
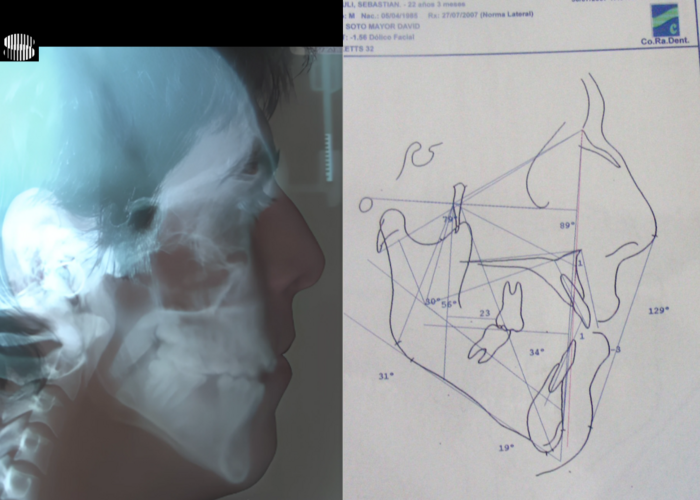
El análisis cefalométrico confirmó una discrepancia esquelética vertical, consistente con una mordida abierta anterior de base esquelética. El plan de tratamiento inicial contemplaba un enfoque ortodóntico-quirúrgico combinado, incluyendo cirugía bimaxilar: osteotomía de impactación tipo Le Fort I y osteotomía sagital bilateral de ramas mandibulares (BSSO), con posible mentoplastia.
Sin embargo, el paciente rechazó la opción quirúrgica y optó por un enfoque puramente ortodóntico, utilizando anclaje esquelético con dispositivos de anclaje temporal (TADs). De este modo, se inició un tratamiento de compromiso, abordando la maloclusión dentro de las limitaciones impuestas por la condición esquelética subyacente del paciente.
Palabra Clave: sagittal osteotomies of the mandible Class II division 1 orthognathic surgery genioplasty
- ABSTRACT
The aim of this clinical case is to demonstrate the correction of an anterior open bite (AOB) with a narrow maxilla in an adult patient, considering the anterior rotational response of the mandible.
A 22-year-old male patient presented to my Orthodontic Clinic with the chief complaint: “I don’t like my smile, and when I speak, I tend to spit… Oh! And I want to be able to bite into an apple,” he said with good humor and positive attitude .
Extraoral clinical examination revealed a vertically long face with an increased lower facial third. The facial profile was slightly convex, with poor chin projection. Intraoral examination showed an AOB and bilateral posterior crossbite.
Cephalometric analysis confirmed a vertical skeletal discrepancy, consistent with a skeletal-based anterior open bite. The initial treatment plan involved a combined orthodontic-surgical approach, including bimaxillary surgery: Le Fort I impaction osteotomy with preliminary surgically assisted maxillary expansion and bilateral sagittal split osteotomy (BSSO), with possible genioplasty.
However, the patient declined the surgical option and opted for a purely orthodontic approach utilizing skeletal anchorage with temporary anchorage devices (TADs). Thus, a compromise treatment plan was initiated, addressing the malocclusion within the constraints imposed by the patient’s underlying skeletal condition.
KEYWORD: sagittal osteotomies of the mandible Open-Bite orthognathic surgery Facial Axis TADs Marpe
- INTRODUCTION
Anterior open bite (AOB) in adults presents one of the most challenging malocclusions in orthodontics, due primarily to its complex etiology, functional implications, and high potential for relapse . AOB is characterized by an absence of vertical overlap between the maxillary and mandibular incisors, while posterior occlusion is often maintained.
The etiology of adult anterior open bite is multifactorial, involving skeletal vertical dimensions, soft tissue function (including tongue posture and lip competence), environmental or habitual influences, and dental-alveolar compensations. Growth completion in adults limits potential for natural skeletal correction, making treatment more dependent on mechanical strategies and/or surgical intervention.
Treatment modalities for adult AOB the biotypology is strongly considered and include orthodontic mechanics such as molar intrusion, incisor extrusion, use of temporary anchorage devices (TADs) ; for more severe skeletal cases, orthognathic surgery is often considered the gold standard to achieve functional and esthetic results.
- CLINICAL AND CEPHALOMETRIC ASSESSMENT




Clinical Findings:
The patient presented with an anterior open bite, characterized by the absence of vertical overlap between the upper and lower incisors, and bilateral posterior crossbite. Extraoral examination revealed a vertically long facial pattern with an increased lower third of the face. The profile is convex with a retruded chin, indicating sagittal and vertical skeletal imbalances. We find also the inclined bipupillary line, which corresponds to facial asymmetries and altered occlusal plane.
Function: Chronic mouth breathers with the distinctive appearance known as adenoid facies , Atypical swallowing with lingual interposition, and phonation patterns related with interposing the tongue between the interincisal opening. The patient also reported functional discomfort when speaking and eating.












Intraoral Examination:
Absent #16, #36 and #46 , No Angle molar relationship . Projection of canines axes in class II relationship . Anterior open bite: Over Bite – 8 mm). Bilateral posterior crossbite: Involvement of upper posterior sectors with inverted buccal-lingual relationship. Moderate Crowding at the level of the upper and lower incisors. Acceptable Oral Hygiene with no periodontal issues
Facial biotype
Algebraic sum (−3,66 ) +(−0,66) + (-2.55) + (-2.55 )+ (-0,5) = − 9, 32 ÷ 5 = -1,84 DOLICHOFACIAL limit severe
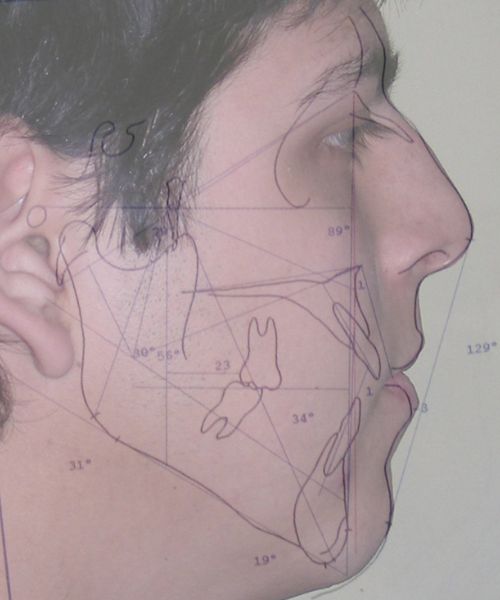
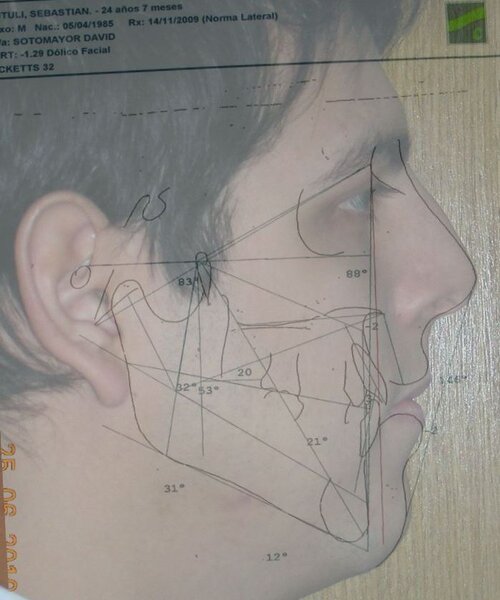
Cephalometric diagnosis
| Parameter | Patient (22yo) | Normal | Interpretation |
|---|---|---|---|
| Facial Axis | 79° | 90° ± 3° | Decreased – indicative of vertical growth pattern– dolichofacial |
| Facial Depth | 89° | 90°± 3° | Slightly reduced (N) – dolichofacial tendency |
| Mandibular Plane Angle | 31° | 22° ± 4° | Increased – dolichofacial tendency |
| Lower Facial Height | 56° | 47 ± 4° |
Increased – long lower third– dolichofacial |
|
Convexity (A–N–Pog) |
+1 mm | ±2 mm | Normal |
| Upper Incisor to A-Pog | 8 mm | 2–4 mm | Proclined upper incisors |
|
Inclination lower Incisor |
19° | 22° | Retroclined lower incisors |
| Interincisal angle | 129° | 130° ± 6° | Decreased – flaring of incisors |
| Maxillary–Mandibular plane angle (MM angle) | 31° | 22° ± 4° | Increased – open bite tendency |
| Mandibular arc | 30° | 31 °± 2 | Slightly reduced– dolichofacial tendency |
| Cranial deflection | 34° | 27° ± 4° | Mildly increased |
Algebraic sum (−3,66 ) +(−0,66) + (-2.55) + (-2.55 )+ (-0,5) = − 9, 32 ÷ 5 = -1,84 DOLICHOFACIAL limit severe
Planning Considerations Following Facial Biotype Assessment
After defining the patient’s facial biotype, we begin to establish a precise pathway for orthodontic planning. The following considerations are fundamental:
1. Cephalometric Parameters Related to Vertical Growth Pattern:
The primary factors directly associated with vertical alterations are the Facial Axis and Lower Facial Height. These measurements are crucial in the assessment and planning of treatment mechanics. As mentioned in previous publications, these vertical discrepancies can be addressed through:
- Intrution of Molars
- Mesialization of posterior segment
A clinical advantage in this case is the absence of three out of four first molars, providing natural space for mesialization mechanics. Additionally, we can utilize temporary anchorage devices (TADs) such as miniscrews, offering enhanced biomechanical control for both intrusion and anchorage reinforcement.
2. Avoid the use of vertical elastics in patients presenting with a dolichofacial pattern and anterior open bite, This critical point is important because they may exacerbate vertical discrepancies.
Treatment plan
-
Perform palatal expansion to address maxillary constriction and correct the posterior crossbite. According to one of the fundamental principles of the bioprogressive philosophy, transverse discrepancies such as crossbites should be addressed before correcting sagittal discrepancies such as overjet
-
Achieve intrusion of the maxillary posterior segments to reduce vertical dimension and promote anterior rotation of the mandible.
-
Plan extraction of #26 after completing palatal expansion then Proceed with mesialization of the posterior segments.
- Alignment, leveling, and coordination of the dental arches in the sagittal, vertical, and transverse planes.
-
Establish anterior guidance by positioning the incisors and canines correctly, ensuring functional disclusion during protrusion and lateral movements.
-
Obtain stable occlusal support on the premolars, contributing to a balanced and functional bite.
-
Apply overcorrection (overtreatment) where needed to anticipate potential relapse and enhance long-term treatment stability.
-
Refer the patient to orofacial myofunctional therapy to address tongue posture, swallowing patterns, and improve overall neuromuscular balance.
-
Design a personalized retention strategy
Treatment phase
At this stage of treatment, following a structured diagnosis and a hierarchically sequenced treatment plan, it is essential to determine the most appropriate treatment mechanics or appliance system to be employed (as previously referenced in the Orthoprogressive introduction ). The success of the treatment is not linked dependent on the type of brackets or aligners used, but rather on the proper diagnosis and application of biomechanical principles.

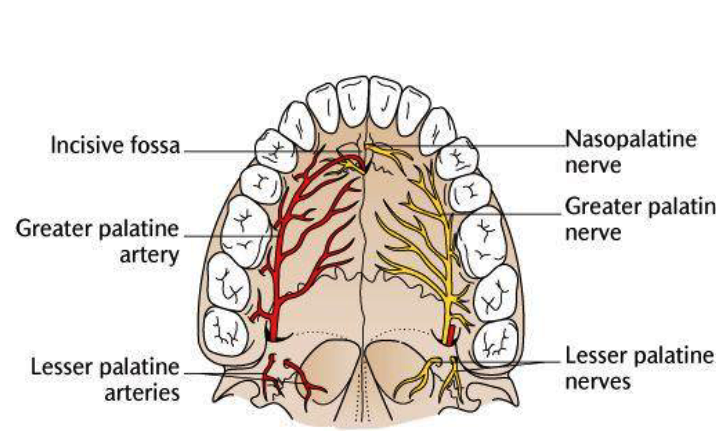
Was installed a Hyrax-type 10mm palatal expander of the Brazilian trademark Morelli® , modified by the author to be adapted to receive TADs microscrews, in order to initiate maxillary disjunction with MARPE (Mini-implant Assisted Rapid Palatal Expansion), TADS was installed with skeletal anchorage placed bilaterally having as references the roots of the maxillary canines and first premolars. Prior to insertion, local infiltrative anesthesia was administered using 2% lidocaine hydrochloride with 1:100,000 epinephrine. A total dose of approximately 0,8 mL per side (cortical infiltration technique). The TADs were inserted under aseptic conditions using a manual driver. Microscrew Evolution 1,6 Ø x 10 mm from the Argentine brand Odontit® . The Hyrax expander was then fitted and activated after 48 hrs .






Protocol of one activation per day was followed for a period of three weeks where the first clinical and radiographic evaluation was performed, showing clear signs of skeletal expansion, including the presence of a midline diastema. One more week of activations was added with a total of 28. The patient reported moderate headache during the first week of activation.
Having successfully achieved the expansion, we proceed to the intrusion of the posterior superior sectors, modifying the Hyrax by adding anchoring hooks at the buccal level of the first premolars. Using the Hyrax as anchorage, we sought a parallel intrusion. This could be replaced by a palatal bar. TADs were installed bilaterally at the mesial level of the first molars, inserting them as parallel as possible to the roots.
Simultaneously we begin with the alignment of the lower arch ,Simultaneously we began with the alignment of the lower arch with Roth prescription ceramic braces .022 . Henry Schein®



 – copia")
As the reader may infer, alignment and leveling of the upper anterior segment are being intentionally deferred at this stage of treatment. This strategic decision is based on the primary objective of closing the anterior open bite not through anterior extrusion, but by means of controlled posterior intrusion. This biomechanical approach promotes a counterclockwise rotation of the mandible, which leads to a increase in the facial axis angle and improvement in vertical facial proportions. By avoiding early anterior alignment, we prevent any premature vertical displacement of the upper incisors.
Clinical changes became evident after 12 months of treatment with posterior intrusion with TADs and nickel-titanium closed coil spring (NiTi), until subsequent follow-up appointments revealed no further significant changes. At that point, it was noted that the most distal molars remained in occlusal contact and had not followed the intrusive movement of their mesial neighbors.







The vertical vector of intrusion was located too far posteriorly to allow for the placement of TADs in that region. At this point, the utility arch developed by Dr. Ricketts was introduced into the mechanics . I referred to as the “Tilting Utility Arch.” made with Blue Elgiloy .017″ × .025″. It was employed as a lever arm to transmit the intrusive force generated by the coil spring and anchored by the TADs.
The upper brackets were bonded solely for the purpose of providing stability to the utility arch . Following the hierarchically structured treatment plan, we proceed with the alignment and leveling phase in order to enable mesialization of the posterior segments using sliding mechanics, which works effectively in conjunction with Roth prescription brackets .022.
A progressive archwire sequence was used for alignment, leveling, and three-dimensional control.
-
.014″ NiTi round wire
-
.016″ NiTi round wire
-
.016″ × .022″ NiTi rectangular wire
- .018″ × .018″ Blue Elgiloy sectional archwire was placed in three segments in the maxillary arch to maximize the effectiveness of Class II intermaxillary elastics, in conjunction with space closure (mesialization) in the mandibular arch.
- 017″ × .025″ Blue Elgiloy sectional leveling archwire beetwen # 35-37 and 45-47
- 017″ × .025″ Stainless Steel (SS) + Closed-coil NiTi springs were activated between the molars and anterior segment
- 019″ × .025″ Stainless Steel (SS)

















After two years of treatment using appropriate biomechanics, the overbite was successfully corrected from -8 mm to +1 mm, achieving complete closure of the anterior open bite without exacerbating the patient’s lower facial third vertical proportions. At this stage, occlusal contacts were verified using articulating paper, and functional movements of the canines and incisors were evaluated to ensure proper anterior guidance and disclusion patterns. The patient was then referred to speech therapy (myofunctional evaluation) as part of the pre-debond assessment protocol.

")
Finishing and Retention




At the completion of treatment (28 months) , the patient exhibited significant skeletal and dental improvements consistent with the initial treatment objectives. A reduction of 3 degrees in lower anterior facial height and a 4-degree increase in the facial axis angle were observed on post-treatment cephalometric analysis, indicating a favorable counterclockwise, anterior mandibular rotation. This skeletal change, in conjunction with the mesialization of posterior segments and space closure mechanics, led to the successful resolution of the anterior open bite. During the retention phase, a modified Hawley appliance was used in the maxillary arch, while the mandibular arch was stabilized with a fixed retainer made of twist-flex (supercable) wire #33 to #43 , which had been heat-treated to eliminate its elasticity. This retention strategy was complemented with myofunctional therapy, aimed at ensuring long-term neuromuscular stability.
The use of cephalometric measurements as quantitative indicators of skeletal and dental movement validated the biomechanical plan established from the outset of treatment. Although the patient maintains a dolichofacial biotype, the desired functional outcome—including anterior occlusal contact, vertical control, and stable mandibular positioning—was effectively achieved.









Regarding the last two photos:
In the first one, the patient—still satisfied after all these years—reached out and sent me this photo to ask about his Hawley retainer that he only uses on weekends and it was in bad shape . He should have been referred earlier to a colleague to replace the appliance, as it had been in use for over 11 years.
In the second photo, I’m sharing experiences with a colleague from Belgium. We were surprised to find incredible similarities in our treatment approaches, especially in how much emphasis we both place on respecting function and biology throughout the orthodontic process.
- CONCLUSIONS
This clinical case demonstrates that anterior open bite correction in an adult patient with skeletal and transverse discrepancies can be successfully achieved through non-surgical orthodontic treatment when a comprehensive and interdisciplinary approach is applied. Despite the initial indication for orthognathic surgery, the patient’s high level of cooperation and the strategic use of skeletal anchorage (TADs) allowed for effective vertical control, posterior intrusion, and anterior guidance reestablishment.
A key factor contributing to the stability of the results was the integration of orofacial myofunctional therapy, which addressed tongue posture, swallowing patterns, and orofacial muscle function. The correction of dysfunctional habits and improvement in orofacial muscle balance played a significant role in minimizing relapse potential and enhancing long-term retention outcomes.
Additionally, a significant improvement in upper airway dimensions was observed following palatal expansion , which may contribute positively to breathing function and overall orofacial health.
This case highlights the importance of patient motivation, individualized treatment planning, and interdisciplinary collaboration—particularly the role of speech therapy—in achieving stable and esthetically pleasing results in non-surgical management of adult anterior open bite.
Completing this case and achieving the planned objectives has been an immensely satisfying experience, both professionally and personally. The clinical progress not only met the functional and esthetic goals, but also reaffirmed the value of Bioprogressive philosophy provided a structured and biologically respectful approach that was key in guiding each decision.
REFERENCES:
1 – American Academy of Oral and Maxillofacial Radiology. Clinical recommendations regarding use of cone beam computed tomography in orthodontics. Position statement by the American Academy of Oral and Maxillofacial Radiology. Oral Surg Oral Med Oral Pathol Oral Radiol. 2013.
2- Iwasaki, T., Saitoh, I., Takemoto, Y., et al. (2014). Tongue posture improvement and long-term stability after maxillary expansion in adults. American Journal of Orthodontics and Dentofacial Orthopedics, 146(5), 600–610.
3- Aljawad, Lee, Lim. PLoS One, 2021. Three‑dimensional evaluation of upper airway changes following rapid maxillary expansion: A retrospective comparison with propensity score matched controls”
4- Gregoret, J., Tuber, E., Escobar, L. H., & Matos da Fonseca, A . Orthodontics and orthognathic surgery: Diagnosis and Planning. Amolca 2014.
5-Kaku, M.; Kawai, A.; Koseki, H.; Abedini, S.; Kawazoe, A.; Sasamoto, T.; Sunagawa, H.; Yamamoto, R.; Tsuka, N.; Motokawa, M.; et al. Correction of severe open bite using miniscrew anchorage. Aust. Dent. J. 2009 , 54, 374–380.
6- Systemized Orthodontic Treatment Mechanics — Richard P. McLaughlin, John C. Bennett, Hugo J. Trevisi. 1ª edición. Mosby, diciembre de 2001
7 – Ricketts RM, Roth RH, Chaconas SJ, Schulhof RJ, Engel GA. Orthodontic diagnosis and planning their roles in preventive and rehabilitative dentistry. 1 ed. Denver: Rocky Mountain; 1982.


